Ca17 Printable Form
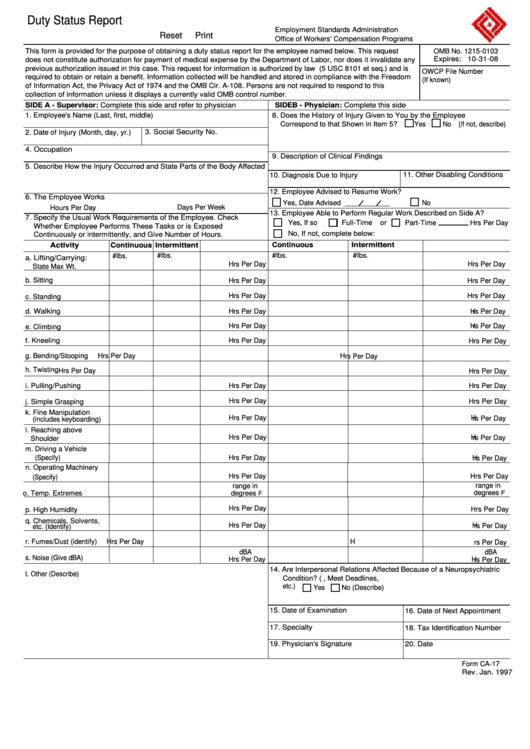
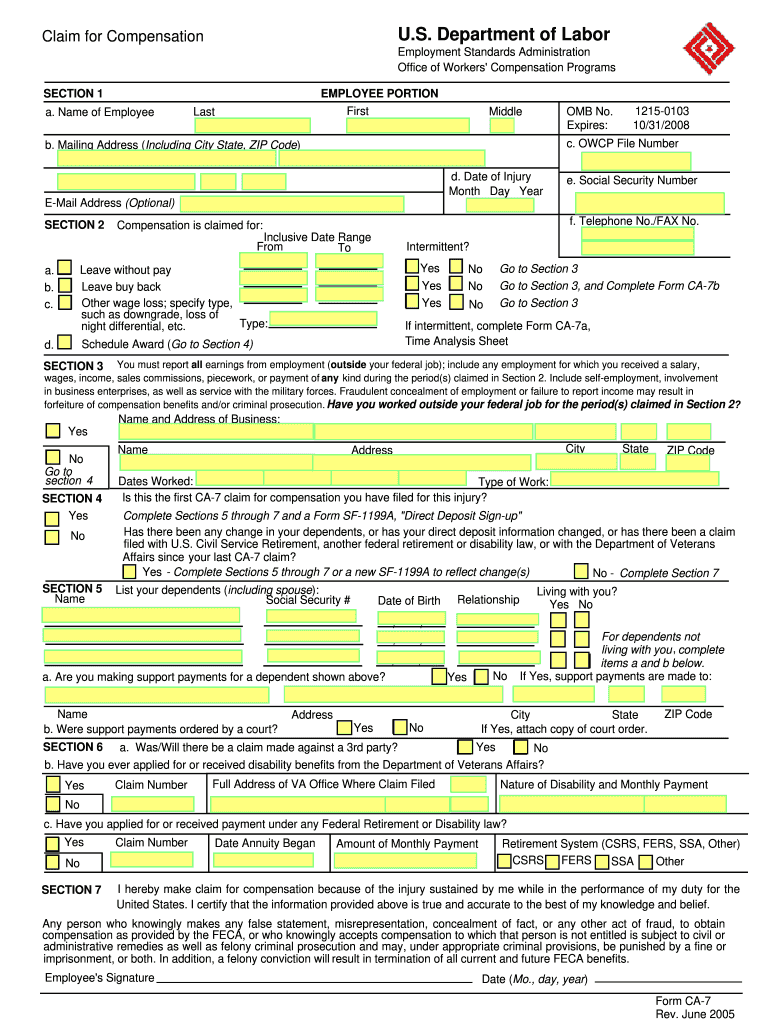
Ca17 Printable Form - Fill in the address of the. Fill in the address of the. Web form number form title elm reference cfc 100 cfc pledge card 617.42 dd 214 certificate of releas e or discharge from active duty. Specify type, yes no go to section 3 such as downgrade, loss of night differential, etc. Web this form provides your supervisor and owcp with interim medical reports containing information as to your ability to return to any type of work. The first side is typically filled in by your supervisor who will indicate the types of actions you carry out. Complete side a and refer the form to the physician. Office of workers' compensation programs. Authorization request form and certification/letter of medical necessity for compounded drugs. Web workers' compensation program forms. Fill in the address of the. Fill in the address of the. Office templates for freegoogle docs for freeexcel templates for free Specify type, yes no go to section 3 such as downgrade, loss of night differential, etc. Authorization request form and certification/letter of medical necessity for compounded drugs. Fill in the address of the. Web form number form title elm reference cfc 100 cfc pledge card 617.42 dd 214 certificate of releas e or discharge from active duty. Office templates for freegoogle docs for freeexcel templates for free Side a, and side b. Complete side a and refer the form to the physician. Fill in the address of the. Fill in the address of the. Web form number form title elm reference cfc 100 cfc pledge card 617.42 dd 214 certificate of releas e or discharge from active duty. Web workers' compensation program forms. Web this form provides your supervisor and owcp with interim medical reports containing information as to your ability to. Fill in the address of the. Complete side a and refer the form to the physician. Office of workers' compensation programs. The first side is typically filled in by your supervisor who will indicate the types of actions you carry out. Web this form provides your supervisor and owcp with interim medical reports containing information as to your ability to. Authorization request form and certification/letter of medical necessity for compounded drugs. Specify type, yes no go to section 3 such as downgrade, loss of night differential, etc. Fill in the address of the. Web form number form title elm reference cfc 100 cfc pledge card 617.42 dd 214 certificate of releas e or discharge from active duty. Web workers' compensation. Office templates for freegoogle docs for freeexcel templates for free 30 day free trialfast, easy & securefree mobile app5 star rated Complete side a and refer the form to the physician. Web form number form title elm reference cfc 100 cfc pledge card 617.42 dd 214 certificate of releas e or discharge from active duty. The first side is typically. Fill in the address of the. Web workers' compensation program forms. Web this form provides your supervisor and owcp with interim medical reports containing information as to your ability to return to any type of work. Office templates for freegoogle docs for freeexcel templates for free The first side is typically filled in by your supervisor who will indicate the. Web workers' compensation program forms. 30 day free trialfast, easy & securefree mobile app5 star rated Fill in the address of the. Office of workers' compensation programs. Fill in the address of the. Authorization request form and certification/letter of medical necessity for compounded drugs. 30 day free trialfast, easy & securefree mobile app5 star rated Office templates for freegoogle docs for freeexcel templates for free Complete side a and refer the form to the physician. Office of workers' compensation programs. Office templates for freegoogle docs for freeexcel templates for free Web this form provides your supervisor and owcp with interim medical reports containing information as to your ability to return to any type of work. Fill in the address of the. Complete side a and refer the form to the physician. Side a, and side b. Web workers' compensation program forms. 30 day free trialfast, easy & securefree mobile app5 star rated Web this form provides your supervisor and owcp with interim medical reports containing information as to your ability to return to any type of work. Specify type, yes no go to section 3 such as downgrade, loss of night differential, etc. Fill in the address of the. Office of workers' compensation programs. Authorization request form and certification/letter of medical necessity for compounded drugs. Side a, and side b. Fill in the address of the. Web form number form title elm reference cfc 100 cfc pledge card 617.42 dd 214 certificate of releas e or discharge from active duty. The first side is typically filled in by your supervisor who will indicate the types of actions you carry out.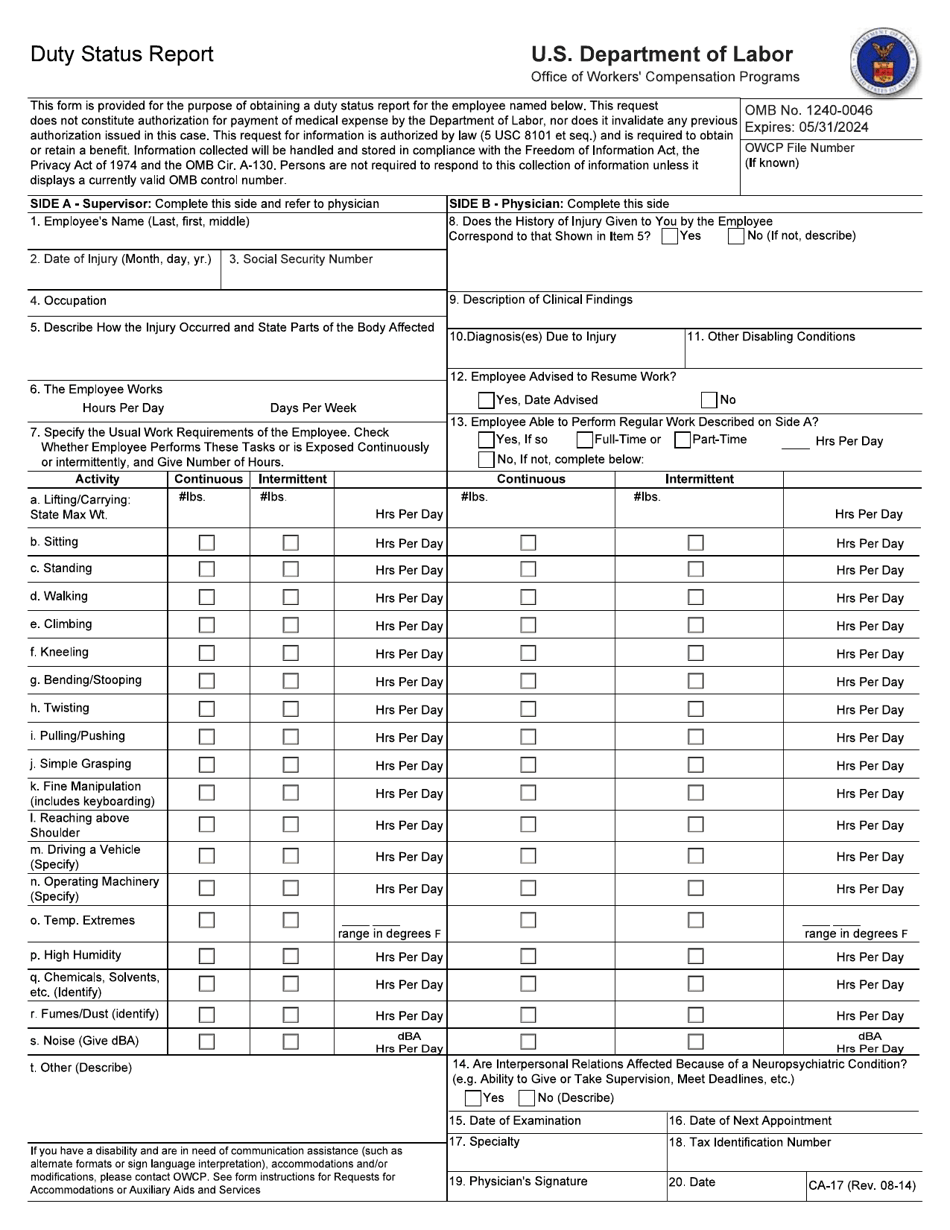
Form CA17 Fill Out, Sign Online and Download Fillable PDF
Printable Ca 17 Form Customize and Print

1997 Form DoL CA16 Fill Online, Printable, Fillable, Blank pdfFiller
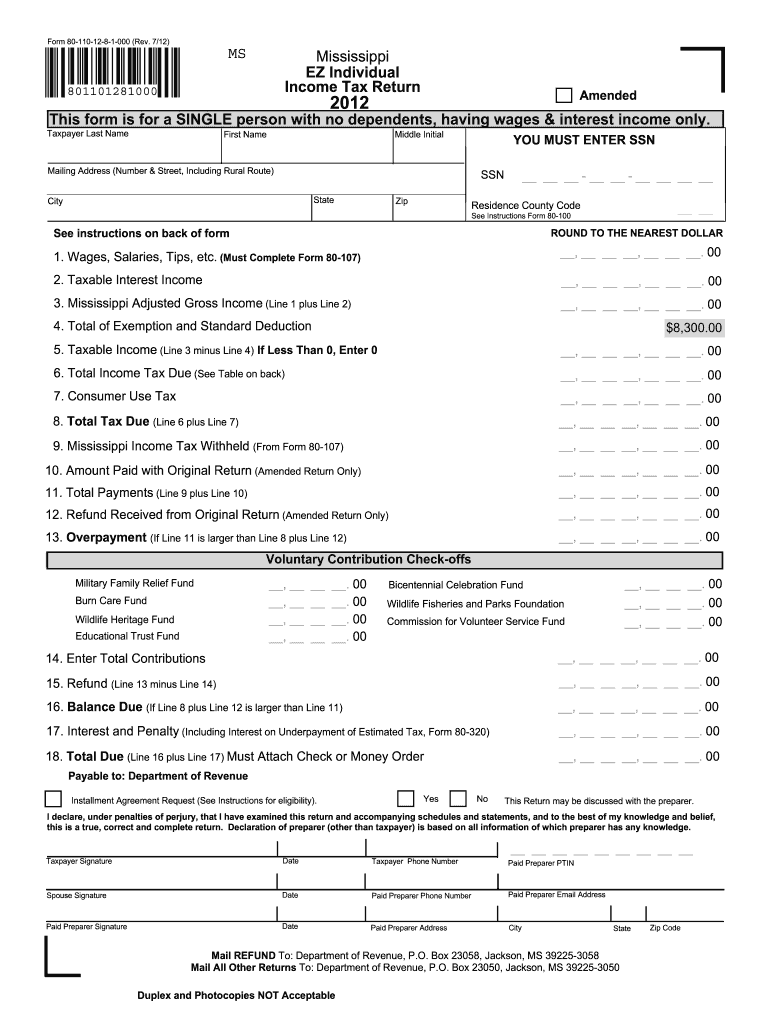
Printable State Tax Forms
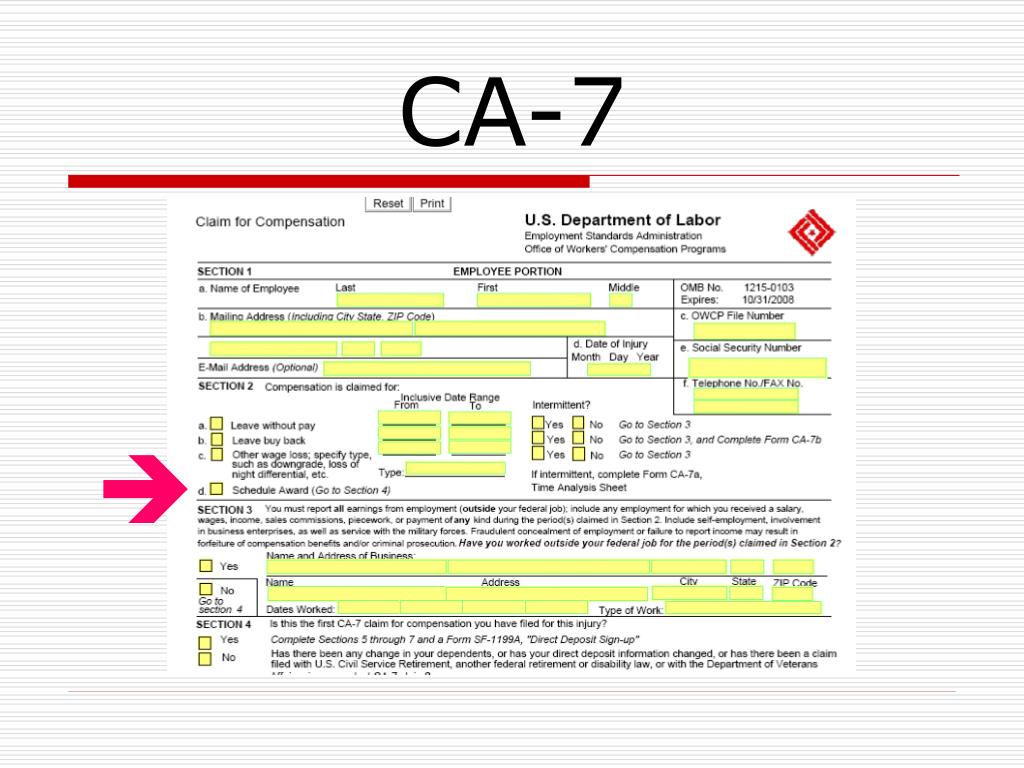
Printable Ca7 Form

CA FL301 20072022 Complete Legal Document Online US Legal Forms
Printable Ca 17 Form Customize and Print
Printable Ca 17 Form
Ca17 Printable Form Printable World Holiday
Print Ca Form 1032 / 2015 Form CA FTB 100S Tax Booklet Fill Online
Fill In The Address Of The.
Office Templates For Freegoogle Docs For Freeexcel Templates For Free
Complete Side A And Refer The Form To The Physician.
Related Post: